
Emerging Insulin Technologies: Redesigning Insulin for the Next Era of Diabetes Care
For over a century, insulin therapy has advanced through refinement of purity, pharmacokinetics, and delivery systems. We are now entering a fundamentally different phase, one focused on redesigning insulin biology itself. Current innovations aim not only to lower glucose but to reduce treatment burden, personalize therapy, and approximate physiologic insulin behavior.
Collectively, these therapies represent a transition from replacement therapy toward engineered metabolic regulation.
Once-Weekly Basal Insulin: Extending Pharmacodynamic Horizons
The most immediately practice-changing development is the emergence of once-weekly basal insulins, including insulin icodec (ONWARDS program) and insulin efsitora alfa (QWINT program).
Across phase 3 trials:
HbA1c reductions were non-inferior — and in some trials superior — to daily basal insulin
Time-in-range improved by ~1 hour/day in insulin-naïve populations
Comparable clinically significant hypoglycemia in type 2 diabetes
Injection burden reduced from 365 to 52 injections/year
In type 1 diabetes, however, higher hypoglycemia rates were observed despite similar HbA1c reductions, raising safety concerns and limiting regulatory approval.
Clinical implication:
Weekly basal insulin may substantially reduce therapeutic inertia and injection resistance, particularly in primary care settings. The challenge shifts toward safe titration during accumulation and integration with CGM-guided care.
Alternative Routes of Administration
Inhaled Insulin
Inhaled Technosphere insulin offers ultra-rapid kinetics with shorter duration than subcutaneous rapid-acting analogs.
Key characteristics:
Slightly less HbA1c reduction vs injected prandial insulin
Comparable achievement of HbA1c targets
Higher patient satisfaction
Pulmonary monitoring required
This therapy occupies a targeted niche: patients prioritizing injection avoidance without pulmonary disease.
Oral Insulin
Several candidates (ORMD-0801, tregopil, capsulin) show modest HbA1c reductions and favorable tolerability, but clinical adoption remains limited by:
Bioavailability <1%
Absorption variability
Inconsistent dose response
The primary research challenge remains achieving predictable pharmacology in the gastrointestinal environment.
Glucose-Responsive Insulin: Toward Autonomous Pharmacologic Regulation
Glucose-responsive insulins are designed to dynamically adjust activity based on ambient glucose concentration. Early models demonstrate reversible receptor binding and glucose-dependent clearance mechanisms in preclinical studies.
If successful, this approach could create pharmacologic closed-loop insulin — biologic automation without external hardware.
No agents are currently available for clinical use, but this remains one of the most transformative research directions in diabetology.
Hepatic Targeting Strategies
Hepato-preferential insulin analogs attempted to mimic portal insulin physiology. Despite promising metabolic effects, development was halted due to hepatic lipid accumulation, enzyme elevation, and inconsistent hypoglycemia patterns.
These findings highlight the complexity of replicating endogenous insulin distribution and reinforce the importance of metabolic safety surveillance in next-generation insulin development.
Patient Selection and Comorbidity Considerations
As insulin platforms become more sophisticated, appropriate patient selection becomes increasingly important.
Pulmonary Disease: Inhaled insulin is contraindicated in asthma and COPD and not recommended in smokers. Spirometry is required before and after initiation. Patients may experience transient cough and small reversible FEV₁ declines.
Type 1 Diabetes: Once-weekly basal insulins demonstrate higher hypoglycemia rates in type 1 diabetes and should be used cautiously. Safety data are reassuring in type 2 diabetes.
Heart Failure: Insulin may exacerbate fluid retention, weight gain, and hypoglycemia — all of which complicate heart failure management.
Cirrhosis: Insulin remains the preferred therapy in decompensated cirrhosis and can be safely used in compensated disease.
Emerging Insulins: Oral and glucose-responsive insulins currently lack defined comorbidity restrictions due to limited clinical exposure.
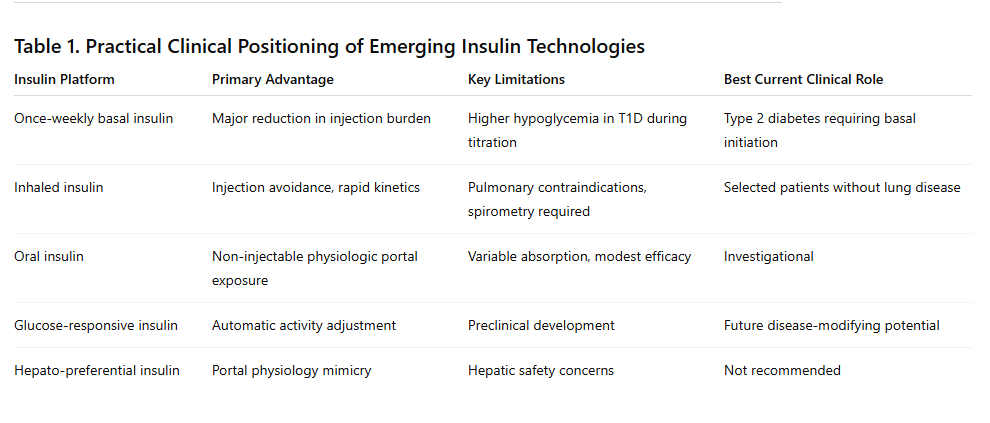
Table 1. Practical Clinical Positioning of Emerging Insulin Technologies
Looking Forward
Insulin innovation is transitioning from longer duration toward biologic intelligence — therapies that adapt, target, and simplify care rather than merely replace deficiency.
For patients, the goal is reduced burden and safer control.
For clinicians, it requires careful selection and new titration strategies.
For researchers, it opens a new field: engineering insulin behavior rather than only modifying pharmacokinetics.
The next frontier in diabetes therapy will not be defined solely by how long insulin lasts, but by how intelligently it works.