
Leveling Up with Incretin Therapy: Expanding Benefits Beyond Diabetes, MACE, and Kidneys
Glucagon-like peptide-1 receptor agonists (GLP-1 RAs) were first introduced as a straightforward tool in the management of type 2 diabetes— what's known in the gaming world as the main storyline quest: improving glycemic control and weight reduction. Soon after, clinicians discovered valuable expansion packs: reductions in major adverse cardiovascular events (MACE) and renal protection. Yet, like any good game, the plot keeps surprising us with new side quests: beyond their established role, GLP-1s are showing potential in areas such as obstructive sleep apnea, physical capacity and musculoskeletal improvements.
With the widespread use of Tirzepatide a dual receptor agonist (GLP/GIP) and the triple agonist Retatrutide anticipated to be on the market in 2027, incretin therapy will likely be the preferred phrasing in the future however for simplicity's sake, this blog post will use the umbrella term GLP-1 RA
Obstructive Sleep Apnea (OSA):
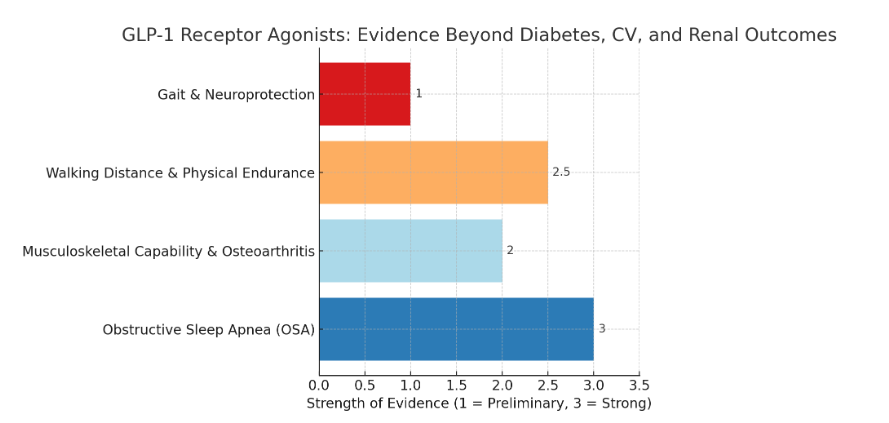
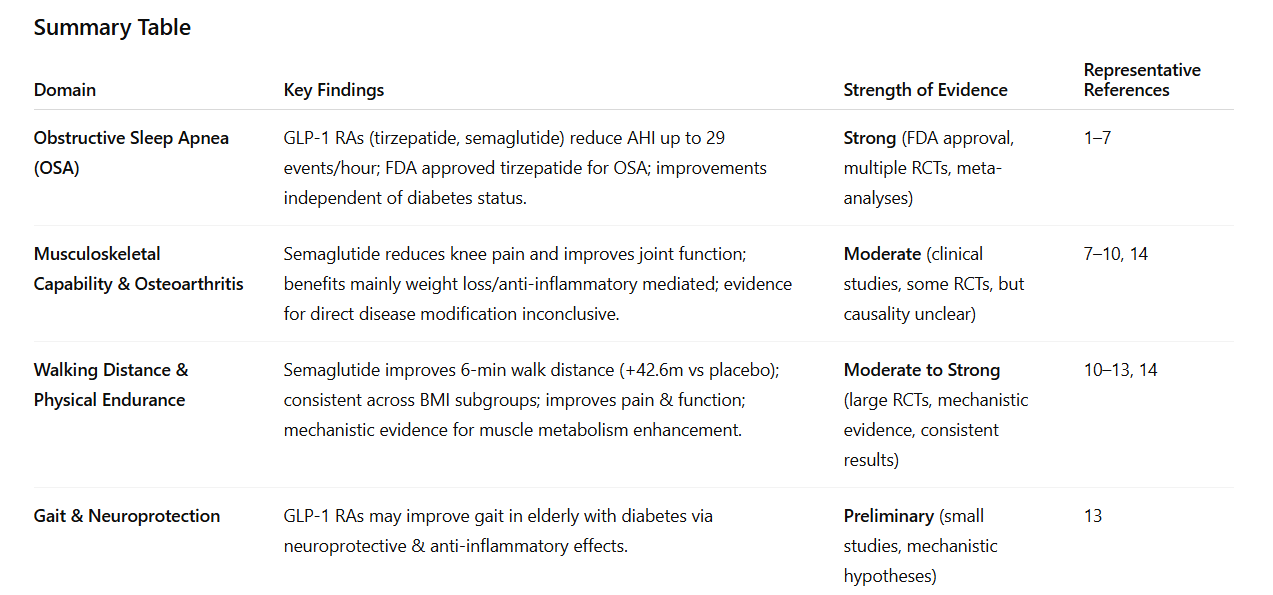
GLP-1 RAs, including Tirzepatide (with the added GIP agonist component) and Semaglutide, significantly reduce the apnea-hypopnea index (AHI) in adults with obesity and moderate-to-severe OSA, with reductions up to 29 events/hour and improvements in sleep-related functioning. These effects are independent of diabetes status and are clinically relevant, as defined by the American Academy of Sleep Medicine. Tirzepatide is now FDA-approved for OSA in adults with obesity, and meta-analyses confirm consistent AHI reductions across multiple randomized controlled trials, though adverse event rates are higher than placebo.[1-6] The Obesity Society also recognizes improvements in OSA as a demonstrated clinical benefit of GLP-1 therapy.[7]
GLP1 Receptor Agonists and the Musculoskeletal System
GLP-1 RAs may improve musculoskeletal function, particularly in knee osteoarthritis, by reducing pain and functional impairment, likely mediated by weight loss and anti-inflammatory effects. Semaglutide has shown benefit in pain reduction and improved joint function in clinical studies, but the evidence for direct disease modification remains inconclusive and is primarily linked to metabolic improvements.[8-10]
Improvements in Physical Endurance with GLP-1 RA's
GLP-1 RAs, specifically Semaglutide, have been shown to improve walking capacity in patients with peripheral artery disease, as demonstrated in the STRIDE trial. Mechanistic studies suggest enhanced skeletal muscle metabolism and endurance via GLP-1R/AMPK signaling, with increased muscle mass and function observed in preclinical models.[10-13] In adults with obesity and knee osteoarthritis, Semaglutide 2.4 mg weekly demonstrated a significant improvement in 6-minute walk distance compared to placebo (mean difference, 42.6 meters; 95% CI, 25.6 to 59.7). Subgroup analyses showed that this improvement was consistent across all baseline BMI categories, indicating benefit regardless of initial obesity severity. The same trial also reported greater improvements in pain and function across BMI subgroups, supporting the generalizability of these findings to the broader obese population with musculoskeletal impairment [13].
Additionally, GLP-1 RAs may improve gait in elderly patients with diabetes, potentially through neuroprotective and anti-inflammatory mechanisms [14].
Summary–Going Further with GLP1 Receptor Agonists
GLP-1 RAs improve OSA severity, musculoskeletal pain and function (especially in osteoarthritis), and walking distance/endurance, with the strongest evidence for OSA and weight-related musculoskeletal improvement. These effects are most pronounced in patients with obesity and are increasingly recognized in clinical guidelines and regulatory approvals.
As the evidence evolves, GLP-1 receptor agonists are proving to be more than just single-mission tools. What began as a diabetes quest now offers physicians a growing set of side quests—cardiovascular, renal, and beyond. The challenge for us is to keep leveling up our knowledge and strategy, so we’re ready when the next expansion pack of data drops.
Stay tuned, because the GLP-1 storyline is still unfolding—and the next side quest may be one your patients are waiting for!
1.Efficacy and Safety of GLP-1 Receptor Agonists in the Management of Obstructive Sleep Apnea in Individuals Without Diabetes: A Systematic Review and Meta-Analysis of Randomized, Placebo-Controlled Trials.Kow CS, Ramachandram DS, Hasan SS, Thiruchelvam K.Sleep Medicine. 2025;129:40-44. doi:10.1016/j.sleep.2025.02.010.
2.Efficacy of Glucagon-Like Peptide-1 Receptor Agonists in Obese or Diabetic Patients With Obstructive Sleep Apnea Syndrome: A Meta-Analysis. Xu S, Li J, Qiu J, et al. Nutrition Reviews. 2025;:nuaf115. doi:10.1093/nutrit/nuaf115.
3.Glucagon-Like Peptide-1 Receptor Agonists for the Treatment of Obstructive Sleep Apnea.D'Annibale DA, Mimoto M, McCowen KC, Malhotra A.Current Opinion in Pulmonary Medicine. 2025;:00063198-990000000-00271. doi:10.1097/MCP.0000000000001208.
4.Glucagon-Like Peptide-1 Receptor Agonists for Obstructive Sleep Apnea in Patients With Obesity and Type 2 Diabetes Mellitus: A Systematic Review and Meta-Analysis.Yang R, Zhang L, Guo J, et al.Journal of Translational Medicine. 2025;23(1):389. doi:10.1186/s12967-025-06302-y.
6.Tirzepatide for the Treatment of Obstructive Sleep Apnea and Obesity. Malhotra A, Grunstein RR, Fietze I, et al.The New England Journal of Medicine. 2024;391(13):1193-1205. doi:10.1056/NEJMoa2404881.
7. Nutritional Priorities to Support GLP-1 Therapy for Obesity: A Joint Advisory From the American College of Lifestyle Medicine, the American Society for Nutrition, the Obesity Medicine Association, and the Obesity Society. Mozaffarian D, Agarwal M, Aggarwal M, et al.The American Journal of Clinical Nutrition. 2025;122(1):344-367. doi:10.1016/j.ajcnut.2025.04.023.
8.Glucagon-Like Peptide-1 (GLP-1) Receptor Agonists in Rheumatology: A Review of Current Evidence and Future Directions.Bilgin E, Venerito V, Bogdanos DP.Autoimmunity Reviews. 2025;24(9):103864. doi:10.1016/j.autrev.2025.103864.
9.The Potential Role of GLP-1 Receptor Agonists in Osteoarthritis.Ryan M, Megyeri S, Nuffer W, Trujillo JM.Pharmacotherapy. 2025;45(3):177-186. doi:10.1002/phar.70005.
10.Impact of Selected Glucagon-Like Peptide-1 Receptor Agonists on Serum Lipids, Adipose Tissue, and Muscle Metabolism-a Narrative Review.Szekeres Z, Nagy A, Jahner K, Szabados E.International Journal of Molecular Sciences. 2024;25(15):8214. doi:10.3390/ijms25158214.
11.GLP-1RAs for Peripheral Artery Disease: A Remarkable STRIDE in the Right Direction.
Verma S, Hess DA.Cell Metabolism. 2025;37(6):1257-1259. doi:10.1016/j.cmet.2025.05.001.
12.GLP-1 Regulates Exercise Endurance and Skeletal Muscle Remodeling via GLP-1R/AMPK Pathway.Wu L, Zhou M, Li T, et al. Biochimica Et Biophysica Acta. Molecular Cell Research. 2022;1869(9):119300. doi:10.1016/j.bbamcr.2022.119300.
13.Research on the Effects of GLP-1 Receptor Agonists in Treating Cognitive Dysfunction and Gait Disorders in Elderly Patients With Diabetes.Yang Y, Chen L, Zhang Y, et al.Frontiers in Pharmacology. 2025;16:1607443. doi:10.3389/fphar.2025.1607443.
14. Once-Weekly Semaglutide in Persons with Obesity and Knee Osteoarthritis.Bliddal H, Bays H, Czernichow S, et al. The New England Journal of Medicine. 2024;391(17):1573-1583. doi:10.1056/NEJMoa2403664.